Orbital Roof Fracture Management

Orbital Roof Fractures A Clinically Based Classification And Treatment Algorithm Omfs

Pdf Early Reconstruction Of Orbital Roof Fractures Clinical Features And Treatment Outcomes Semantic Scholar

Facial Fractures Earwell Center Of Excellence

Pdf Traumatic Orbital Roof Fractures Interdisciplinary Evaluation And Management

Figure 1 From Natural Course Of Orbital Roof Fractures Semantic Scholar

Figure 4 From Reconstruction Of Orbital Roof Fracture Using Titanium Mesh Case Report And Review Of Literature Semantic Scholar
However intracranial or intraorbital injury may warrant surgical intervention to remove impinging bony fragments repair dura or reconstruct the orbital roof.
Orbital roof fracture management.

Diagnosis And Imaging Of Orbital Roof Fractures A Review Of The Current Literature Semantic Scholar
Orbital Roof Blow In Fracture A Case Report And Review Jones Journal Of Radiology Case Reports
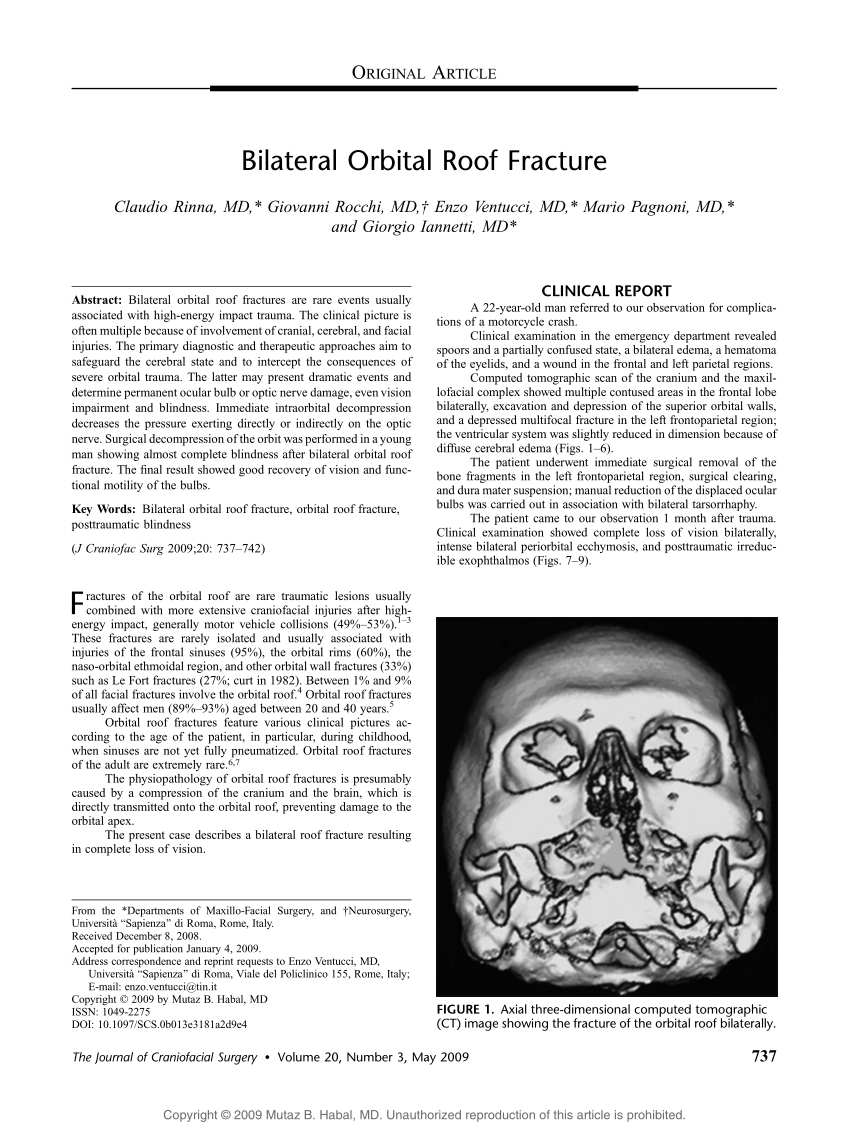
Pdf Bilateral Orbital Roof Fracture

Isolated Orbital Roof Fracture Can It Be Catastrophic Sadashivam S Asian J Neurosurg
Open Treatment For Orbit Orbital Roof Fracture
Diagnosis And Treatment Of Orbital Fractures

Figure 6 From Orbital Fractures Role Of Imaging Semantic Scholar

Figure 4 From Orbital Roof Blowin Fracture A Case Report And Review Semantic Scholar

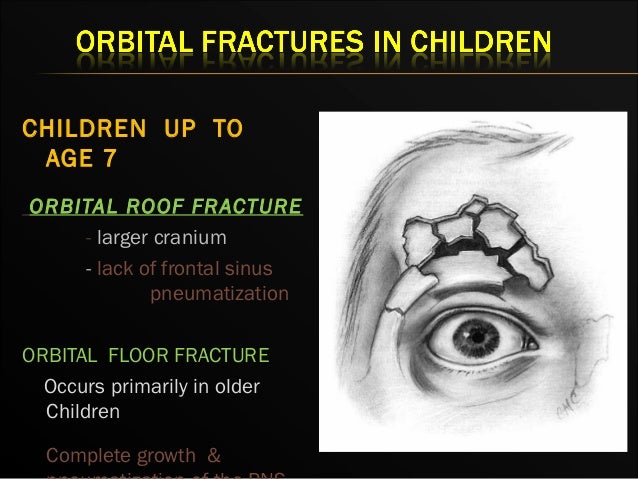
Aaps Twenty Years Of Pediatric Orbital Roof Fractures Incidence Patterns And Indications For Operation
Pdf Titanium Mesh Reconstruction Of Orbital Roof Fracture With Traumatic Encephalocele A Case Report And Review Of Literature

Table 5 From Orbital Roof Fractures A Clinically Based Classification And Treatment Algorithm Semantic Scholar
Orbital Fracture
Https Www Ajronline Org Doi Pdf 10 2214 Ajr 139 5 969
Orbital Apex And Roof Fractures American Academy Of Ophthalmology

Bilateral Blow In Fractures Of Orbital Roofs Download Scientific Diagram

Orbital Roof Blowin Fracture A Case Report And Review Semantic Scholar
Https Www Sciencedirect Com Science Article Pii S1071094998800371 Pdf Md5 94635eed83a50be3da7f9e496984580f Pid 1 S2 0 S1071094998800371 Main Pdf

T2gre Coronal Mr Image Shows Fracture Through Cribriform Plate And Download Scientific Diagram
Https Encrypted Tbn0 Gstatic Com Images Q Tbn 3aand9gcqycbcdgoe6rzb6oic0fdozorujti4io1tvpnsexbak2qbljwr3 Usqp Cau

Orbital Blowout Fracture Radiology Reference Article Radiopaedia Org

Pdf Bilateral Blow In Fractures Of The Orbital Roofs Caused By The Ballistic Effect Of A High Velocity Stone An Unusual Presentation Of Orbital Trauma Semantic Scholar
Pdf Pearls Of Orbital Trauma Management

Pediatric Facial Fractures Children Are Not Just Small Adults Radiographics
Orbital Fractures
Source : pinterest.com
