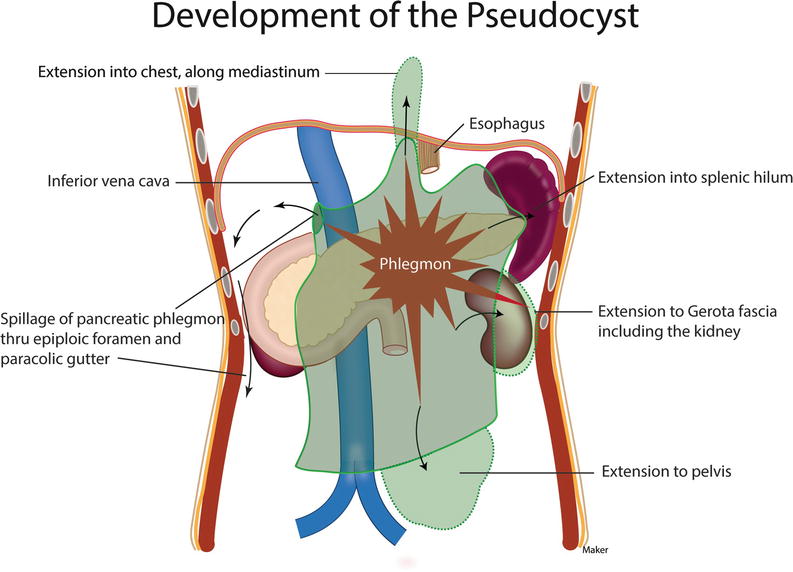
Pancreatic Drainage Into Paracolic Gutter

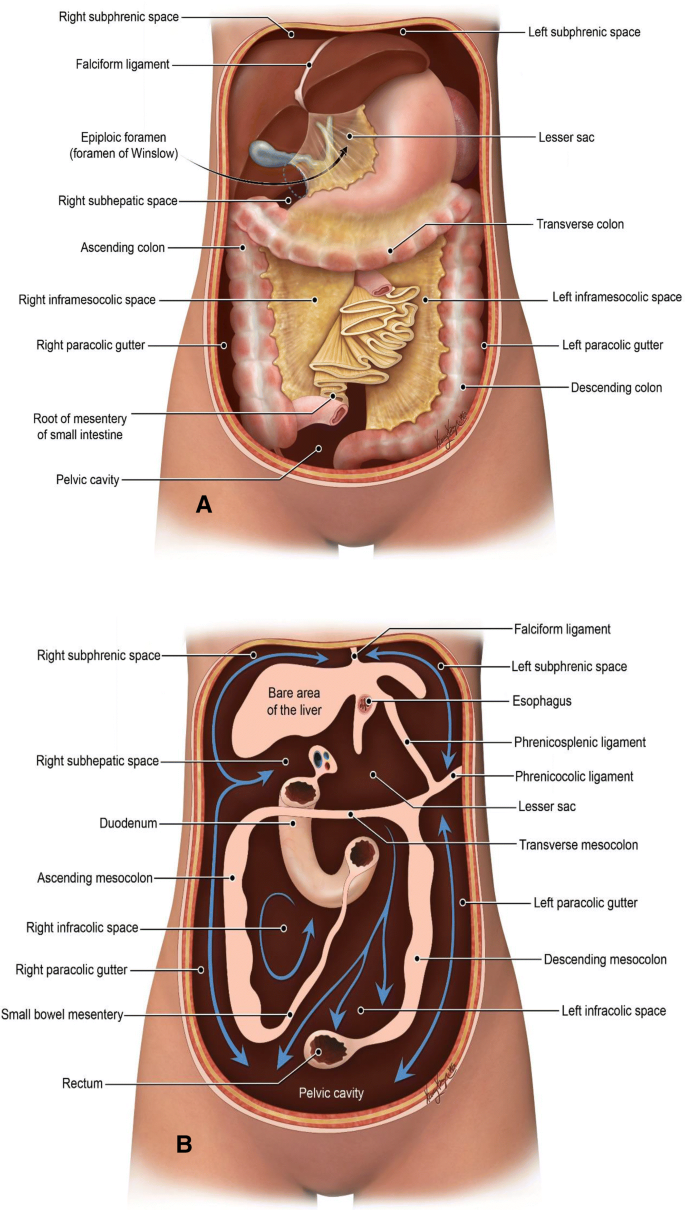
The Peritoneal Cavity Greater Sac Lesser Sac Teachmeanatomy

Stomach In Situ Anatomy Falciform Ligament Gallbladder Pylorus Caudate Lobe Of Liver Duodenum Left Lobe Of Liv Anatomy Liver Anatomy Gallbladder
Http Pdf Posterng Netkey At Download Index Php Module Get Pdf By Id Poster Id 133725
Http Pdf Posterng Netkey At Download Index Php Module Get Pdf By Id Poster Id 114921

Abdominal Wall Mesentery Peritoneum And Vessels Radiology Key
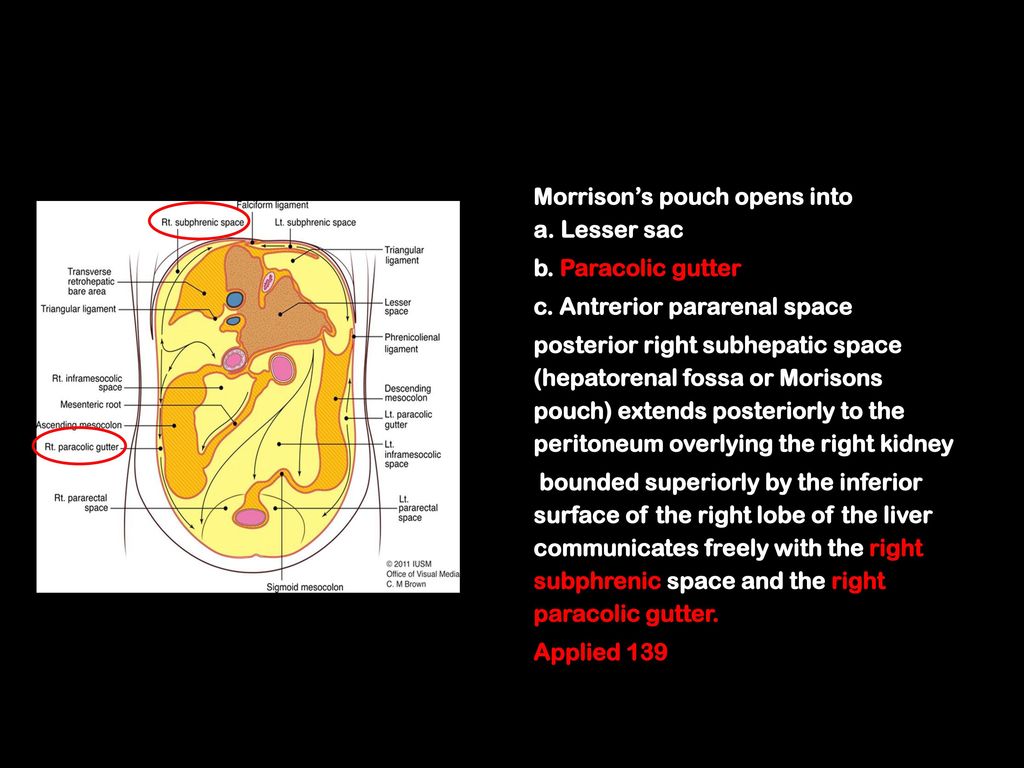
Morison S Pouch Anatomical Review And Evaluation Of Pathologies And Disease Spread On Cross Sectional Imaging Springerlink

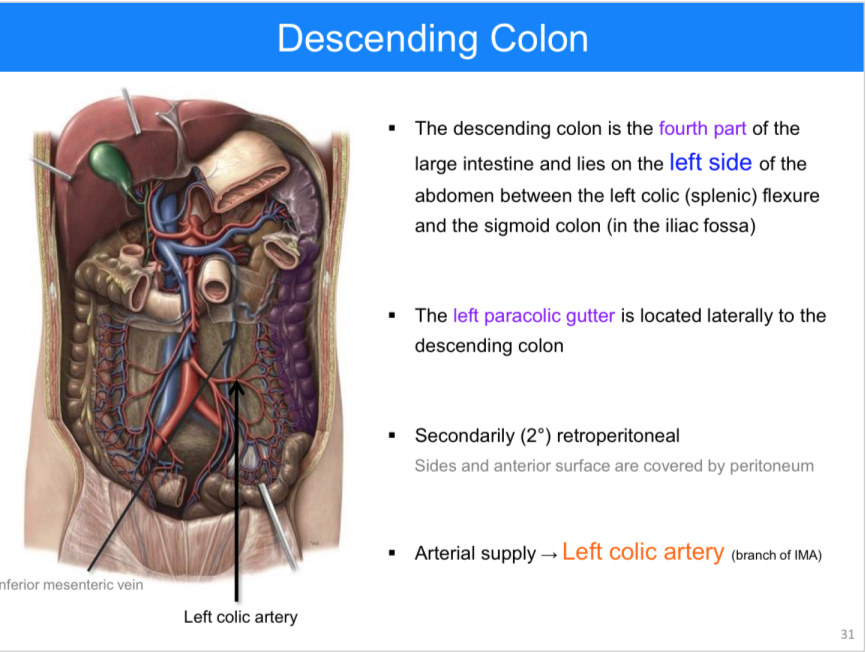
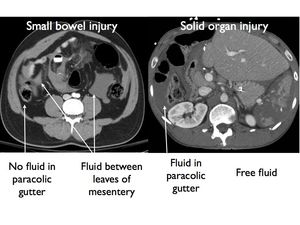
The right and left paracolic gutters are peritoneal recesses on the posterior abdominal wall lying alongside the ascending and descending colon.
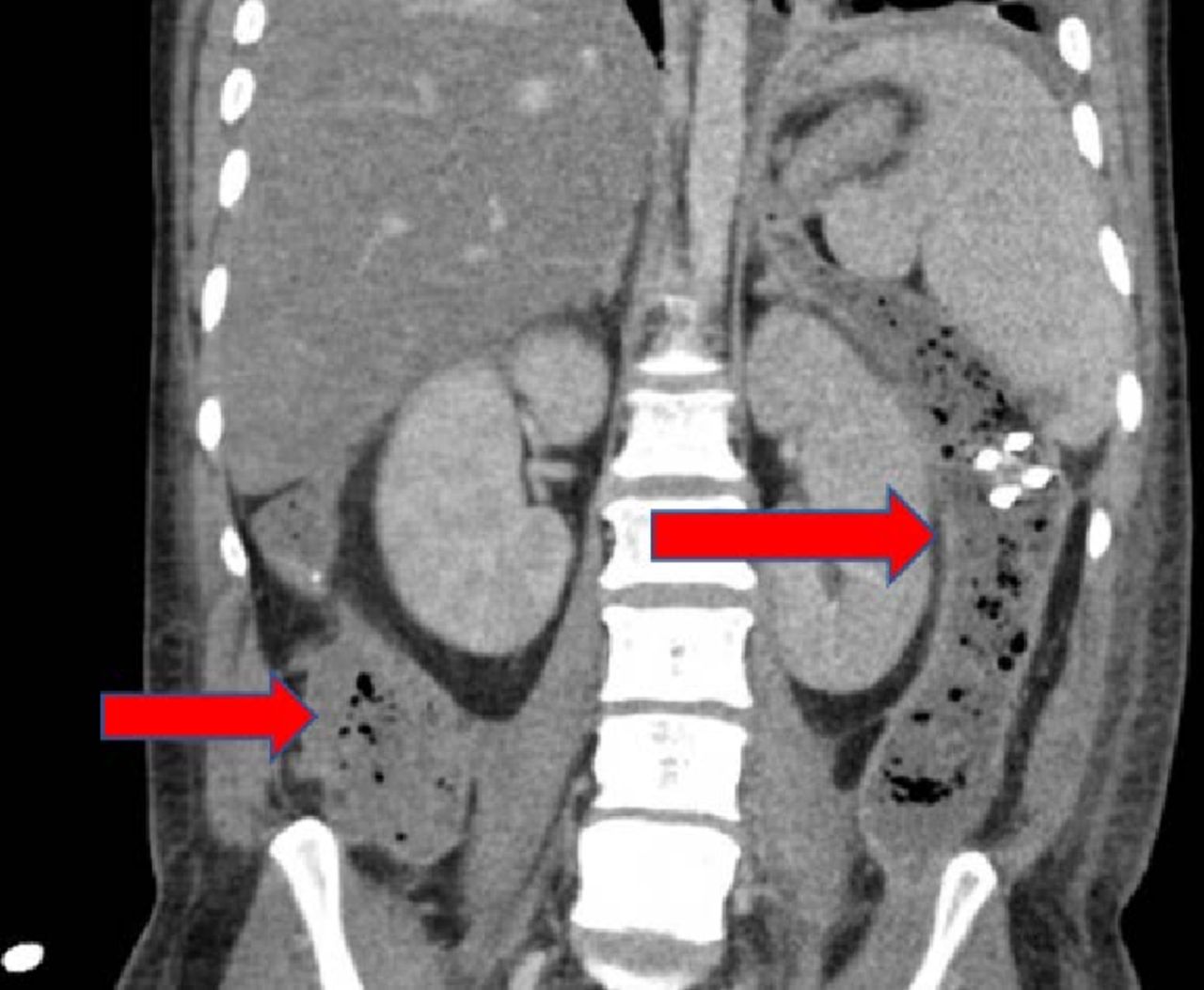
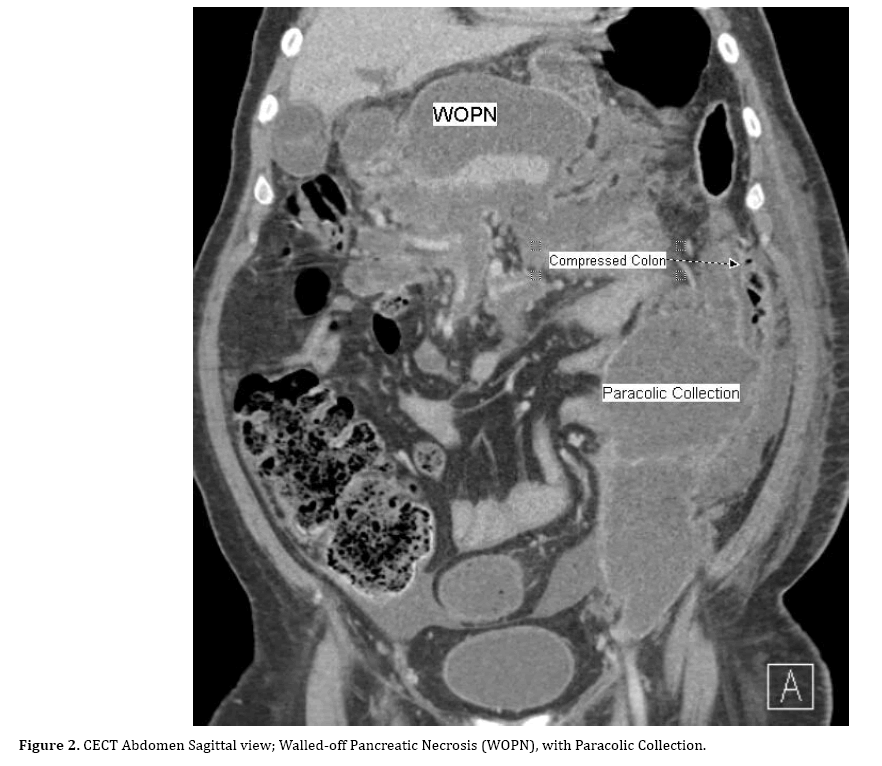
Pancreatic drainage into paracolic gutter.

Ct Showing Free Fluid In The Right Paracolic Gutter No Free Air And Download Scientific Diagram
Step Up Approach For The Management Of Pancreatic Necrosis A Review Of The Literature Tsaco
The Peritoneum What Nuclear Radiologists Need To Know Sciencedirect

Variations In Colic Arteries Anatomy Middle Colic Artery Right Colic Artery Ileocolic Artery Common Trunk For Rig Arteries Anatomy Arteries Colic
Pancreas Springerlink

Structure Of Paracolic Gutter Body Structure Semantic Scholar
Anatomy Of The Abdomen 3 Infracolic Viscera Anatomy Flashcards Memorang

Ct Scan Visualizes A Large Fluid Collection Fc In The Retroperitoneal Download Scientific Diagram

Pin De Michele Vitoria Em Modulo Gastrointestinal Sistema Linfatico Linfatica Nervos

Urinary Bladder Female And Male Anatomy Female Frontal Section Parietal Peritoneum Fundus Of Bladder Interurete Bladder Shoulder Muscle Anatomy Anatomy
Https Pubs Rsna Org Doi Pdf 10 1148 Rg 254045035
Https Link Springer Com Content Pdf 10 1007 2f978 1 4757 3958 9 2 Pdf
Https Sonomir Files Wordpress Com 2013 01 Fast Protocol Pdf

Lymph Vessels And Nodes Of Small Intestine Anatomy Thoracic Duct Cisterna Chyli Intestinal Lymphatic Tr Intestines Anatomy Lymph Vessels Thoracic Duct
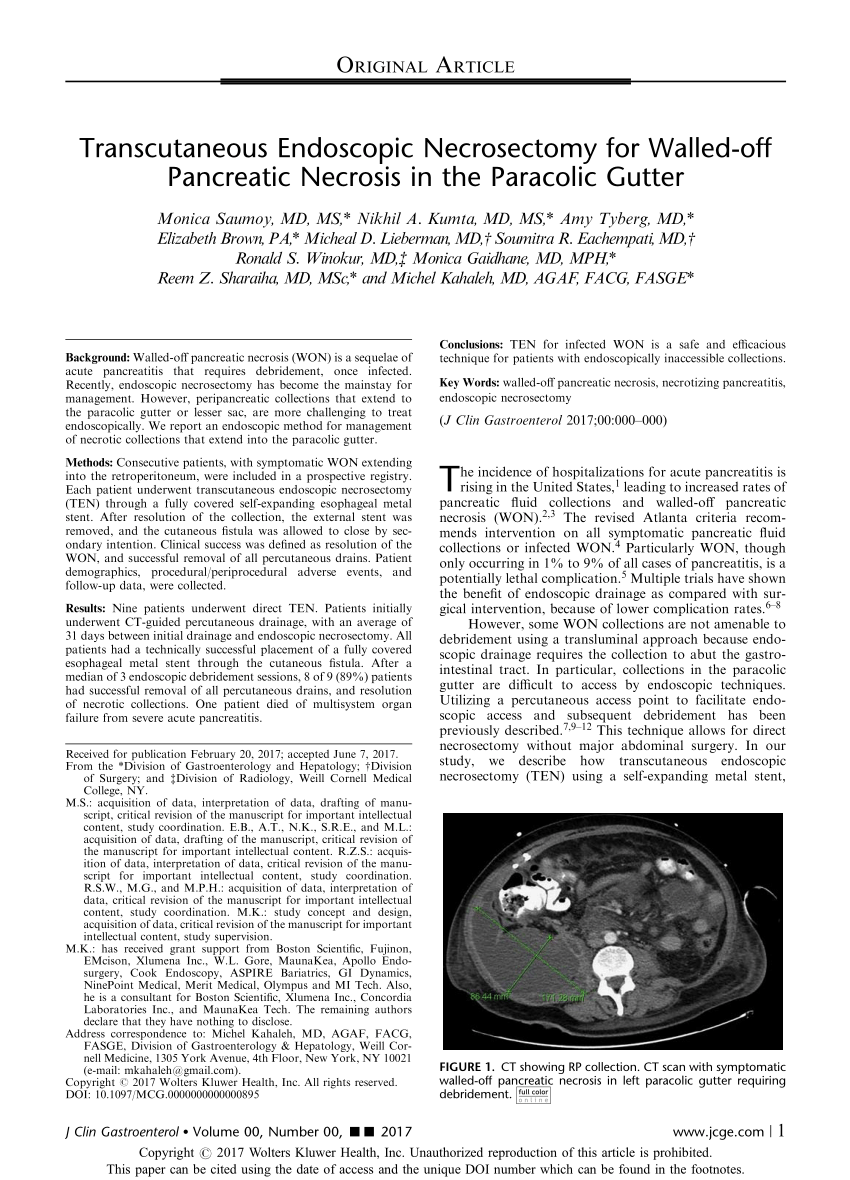
Pdf Transcutaneous Endoscopic Necrosectomy For Walled Off Pancreatic Necrosis In The Paracolic Gutter
Abdomen Nontraumatic Emergencies Radiology Key
Multiple Pancreaticocolonic Fistulas Involving The Transverse And Descending Colon With Multiple Walled Off Pancreatic Necroses Reporting Of A Complex Case Treated Surgically Insight Medical Publishing
Epos
Https Encrypted Tbn0 Gstatic Com Images Q Tbn 3aand9gcsz2 Jmhhn3hfet5i4xlbnkwzbuxksu2gxpznr57ucykitv2nnz Usqp Cau
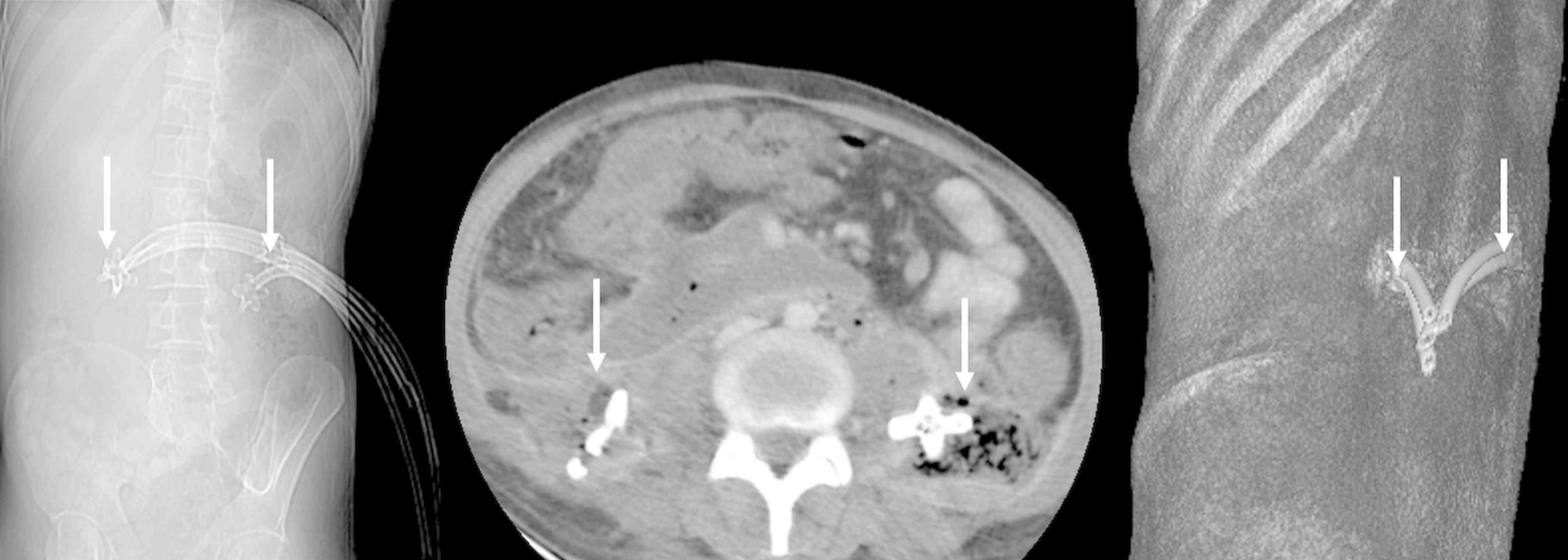
Kissing Catheter Technique For Percutaneous Catheter Drainage Of Necrotic Pancreatic Collections In Acute Pancreatitis
Dr Ibtisam Musallam Aljohani Kamc Ppt Download
Https Www Research Manchester Ac Uk Portal Files 102607496 Full Text Pdf

Short Term Outcome Of Local Pancreatic Complications In A Public Hospital From North India Postgraduate Medical Journal

The Abdominal Wall And Peritoneal Cavity Radiology Key
Source : pinterest.com
